

Diverting least-sick patients from ER looks good, accomplishes little

Advertisement
Read this article for free:
or
Already have an account? Log in here »
To continue reading, please subscribe:
Monthly Digital Subscription
$0 for the first 4 weeks*
- Enjoy unlimited reading on winnipegfreepress.com
- Read the E-Edition, our digital replica newspaper
- Access News Break, our award-winning app
- Play interactive puzzles
*No charge for 4 weeks then price increases to the regular rate of $19.00 plus GST every four weeks. Offer available to new and qualified returning subscribers only. Cancel any time.
Monthly Digital Subscription
$4.75/week*
- Enjoy unlimited reading on winnipegfreepress.com
- Read the E-Edition, our digital replica newspaper
- Access News Break, our award-winning app
- Play interactive puzzles
*Billed as $19 plus GST every four weeks. Cancel any time.
To continue reading, please subscribe:
Add Free Press access to your Brandon Sun subscription for only an additional
$1 for the first 4 weeks*
*Your next subscription payment will increase by $1.00 and you will be charged $16.99 plus GST for four weeks. After four weeks, your payment will increase to $23.99 plus GST every four weeks.
Read unlimited articles for free today:
or
Already have an account? Log in here »
Hey there, time traveller!
This article was published 23/01/2024 (688 days ago), so information in it may no longer be current.
Manitoba’s largest hospital is gathering some useful data that will likely show how diverting low-acuity patients away from emergency departments has virtually no impact on overall ER wait times.
It seems this new data is necessary to prove, once again, that removing some of the least sick people from ERs does not solve the problem of long ER wait times.
Why are they doing this again after multiple Canadian studies have shown it has little to no impact on ER wait times? Because health care in Canada is driven more by politics than evidence-based decision making.
Politicians need quick, easy-to-grasp solutions to create the impression they’re doing something to improve health-care outcomes. Diverting low-acuity patients from ERs to minor treatment clinics, or elsewhere, is the quickest and least costly way to achieve that, even though it doesn’t reduce overall wait times.
Last week, Health Minister Uzoma Asagwara announced an additional doctor has been hired to staff the minor treatment clinic at Health Sciences Centre. The move is being hailed as a way of reducing ER wait times.
On its face, it seems to make sense. Take the least sick people out of ER waiting rooms — the ones who could have been treated at a walk-in clinic or by their family doctor — and there will be fewer people lined up to see an ER physician. The fewer people waiting for treatment, the shorter the wait times. Or so goes the political argument.
Trouble is, in the real world of medicine, it doesn’t work that way. Multiple studies over the past several decades (see the Canadian Association of Emergency Physicians for details) have shown diverting low-acuity patients from ERs has a negligible impact on ER wait times.
The main reason is that low-acuity patients — people with broken toes, earaches, etc. — are not typically sick enough to be admitted to hospital.
They wait longer to see an ER physician than those who are sick enough to require a hospital bed. That’s how the triage system works and should work. But reducing the number of those patients in ER waiting rooms has very little impact on overall wait times, studies have shown.
The main reason is because it’s the sicker ER patients, those who require a hospital bed but can’t get one because there isn’t one available, that drive up ER wait times the most, studies show.
The greater the number of admitted patients piling up in emergency departments (there are record numbers of them in Winnipeg hospitals these days) the more time ER docs and nurses spend treating them and the less time they have to see new patients. That drives up overall wait times.
Taking away the broken-toe and earache patients does nothing to alleviate that congestion.
The statistics prove it. HSC will need more data over a longer period of time to draw definitive conclusions on its latest minor treatment clinic experiment. But so far — despite claims to the contrary — the clinic has done nothing to reduce ER wait times.
Between August (when the clinic was created) and November, ER wait times at HSC soared to record levels. The longest wait time for nine out of 10 patients (the 90th percentile) jumped from 11.4 hours to 13.75 hours during that period. The median wait time increased from 3.4 hours to 3.9 hours.
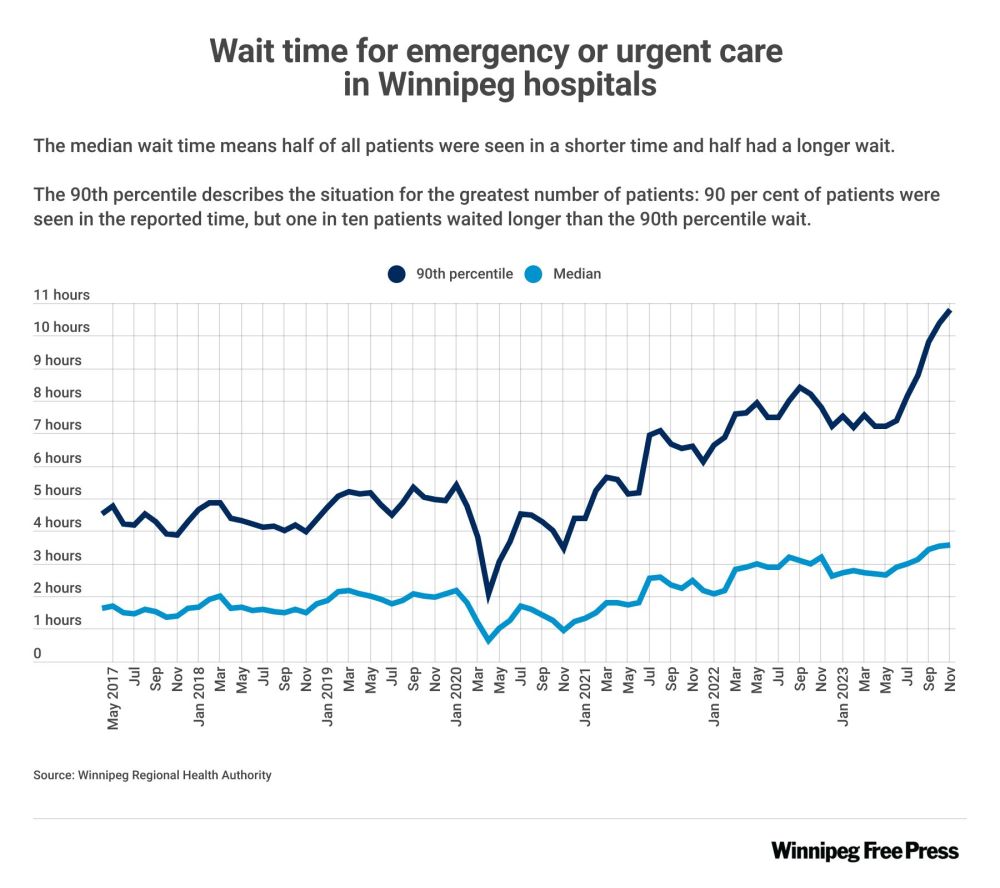
Granted, those numbers coincide with the rise in respiratory illness season, when ER wait times typically rise. But there is no evidence the minor treatment clinic has had any impact on overall waits.
That’s because while more than 2,000 low-acuity patients have been diverted from the ER to the minor treatment clinic during that period, the number of admitted patients in the ER continues to rise.
Why? Because there aren’t enough staffed medical beds in the system to accommodate them. It’s a hospital overcrowding problem, not a case of too many low-acuity patients showing up at ERs.
Did those 2,000-plus low-acuity patients get speedier care by going to a clinic instead of an ER? Sure. But some, maybe most, of them could have done so on their own.
More important, it did nothing to solve the crisis. Doing so is a lot more costly and complicated than diverting a few thousand broken-toe patients away from ERs. That’s why politicians and senior health-care bureaucrats prefer to focus on low-acuity patients than sicker ones. It’s an easy sell to the public. It gives the impression that government is doing something about a high-profile problem.
Governments of all political stripes are guilty of this smoke-and-mirrors approach. Both the former Progressive Conservative government and the NDP before them did it. The result: ER wait times have nearly doubled over the past decade.
That won’t change — no matter how many minor treatment clinics they open — until they address the root cause of the problem: hospital overcrowding and all of the complexities that go into solving it.
tom.brodbeck@freepress.mb.ca
Tom Brodbeck is an award-winning author and columnist with over 30 years experience in print media. He joined the Free Press in 2019. Born and raised in Montreal, Tom graduated from the University of Manitoba in 1993 with a Bachelor of Arts degree in economics and commerce. Read more about Tom.
Tom provides commentary and analysis on political and related issues at the municipal, provincial and federal level. His columns are built on research and coverage of local events. The Free Press’s editing team reviews Tom’s columns before they are posted online or published in print – part of the Free Press’s tradition, since 1872, of producing reliable independent journalism. Read more about Free Press’s history and mandate, and learn how our newsroom operates.
Our newsroom depends on a growing audience of readers to power our journalism. If you are not a paid reader, please consider becoming a subscriber.
Our newsroom depends on its audience of readers to power our journalism. Thank you for your support.
Tom Brodbeck is an award-winning author and columnist with over 30 years experience in print media. He joined the Free Press in 2019. Born and raised in Montreal, Tom graduated from the University of Manitoba in 1993 with a Bachelor of Arts degree in economics and commerce. Read more about Tom.
Tom provides commentary and analysis on political and related issues at the municipal, provincial and federal level. His columns are built on research and coverage of local events. The Free Press’s editing team reviews Tom’s columns before they are posted online or published in print – part of the Free Press’s tradition, since 1872, of producing reliable independent journalism. Read more about Free Press’s history and mandate, and learn how our newsroom operates.
Our newsroom depends on a growing audience of readers to power our journalism. If you are not a paid reader, please consider becoming a subscriber.
Our newsroom depends on its audience of readers to power our journalism. Thank you for your support.
Related Articles
Health-care overhaul can’t stay on hold






Advertisement Advertise With Us
Advertisement Advertise With Us
History
Updated on Wednesday, January 24, 2024 10:05 AM CST: Updates chart